AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8965/044
Department of Surgery, Anorectal Physiology Laboratory, University Medical Center Groningen, 1 Hanzeplein, PO Box 30 001, 9700 RB Groningen, the Netherlands
*Corresponding Author: Aia Al-Saidi, Department of Surgery, Anorectal Physiology Laboratory, University Medical Center Groningen, 1 Hanzeplein, PO Box 30 001, 9700 RB Groningen, the Netherlands
Citation: Aia Al-Saidi, Ellen R. Klinkert, Sijbrand Hofker, Monika Trzpis, Paul M.A. Broens. (2020) Suboptimal Bowel Function after (Recto) Sigmoid Resection in Patients with Deep Infiltrating Endometriosis. J Obstetrics Gynecology and Reproductive Sciences, 4(2): DOI: 10.31579/2578-8965/044
Copyright: © 2020. Aia Al-Saidi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 July 2020 | Accepted: 06 August 2020 | Published: 10 August 2020
Keywords: defecation; fecal incontinence; constipation; irritable bowel syndrome; deep infiltrating endometriosis
Purpose: To investigate the postoperative outcomes regarding bowel functions in women and the pattern of symptoms after surgical treatment for deep infiltrating endometriosis in comparison with healthy subjects.
Methods: This cross-sectional study was designed as a single tertiary-level academic center. We included 130 female adult patients who had undergone (recto) sigmoid resection for deep infiltrating endometriosis between January 2005 and December 2015. Patients were randomly age-matched to two controls derived from the general population in the Netherlands. We measured the prevalence of constipation, fecal incontinence, Irritable Bowel Syndrome and the Low Anterior Resection Syndrome Score.
Results: The prevalence of constipation, fecal incontinence, and irritable bowel syndrome in the patients was significantly higher than in the controls (50.8% versus 26.2% and 15.4% versus 5.4%, and 14.6% versus 5.4%, respectively, P < 0.05 for each). The prevalence of constipation and fecal incontinence was lower in the patients who had undergone surgery longer than 24 months ago, in comparison with those who had undergone surgery less than 24 months ago (46.7% versus 69.9% and 15.0% versus 17.4%), which was still significantly higher in comparison to the control group. The low anterior resection syndrome score was significantly higher in the patients than in the controls.
Conclusion: The postoperative outcomes in patients treated for deep infiltrated endometriosis regarding constipation, fecal incontinence, and irritable bowel syndrome are suboptimal and do not come close to outcomes in the general female population in the Netherlands. These patients should be screened postoperatively and if necessary, treated for bowel functions.
Deep infiltrating endometriosis (DIE) is often associated with functional disorders of muscles and organs located in the pelvic floor [1-3]. Chronic pelvic pain, dyspareunia, infertility, increased pelvic floor muscle spasms, and altered bowel habits are common symptoms [4-6]. As a result of the overgrowth of endometriosis different physiological processes in the pelvic floor may also become impaired, leading to problems such as constipation, fecal incontinence (FI), and irritable bowel syndrome (IBS) [7-9]. Previous publications already showed that women with DIE report significant postoperative improvement of their bowel functions after surgical removal of the DIE [10, 11] in comparison to preoperative conditions. Such findings could, however, give patients the vain hope that their health will be restored to the same state as before they fell ill, especially when taking into account that most improvement is based on pain reduction. We know, however, that patients who underwent surgical treatment for DIE still tend to experience pelvic floor muscle tenderness [12] that can give rise to symptoms other than pain. A previous report stated that segmental bowel resection for DIE might be associated with an increased incidence of new bowel symptoms, as a result perhaps of abdominal pain and incomplete bowel movements [13]. Based on our clinical experience, we know that despite postoperative improvement of bowel functions, patients’ bowel functions are still far from optimal. The question is, how far.
To answer this question, we aimed to assess whether frequency and magnitude of defecatory disorders in patients who underwent (recto) sigmoid resection for DIE were comparable to women who never had DIE. We compared the prevalence and odd ratios of defecatory disorders and the spectrum and pattern of their symptoms in patients and women from the general Dutch population who had never undergone surgery and/or had no comorbidities that could influence defecation and fecal continence.
Study design
This cross-sectional study was designed as a single-center study and was performed at the Department of Gynecology in cooperation with the Abdominal Surgery and the Anorectal Physiology Laboratory, both of the Department of Surgery at the University Medical Center of Groningen, the Netherlands.
Defec Questionnaire
The postoperative evaluation of the fecal problems was performed using
the validated Groningen Defecation & Fecal Continence questionnaire (DeFeC) [14]. The questionnaire contains questions on demographic issues, symptoms related to constipation, FI and IBS, medical history, and diet. It also contains questions based on the Rome IV criteria for constipation, FI and IBS. The patients and the control group received the same DeFeC questionnaire.
Patient group
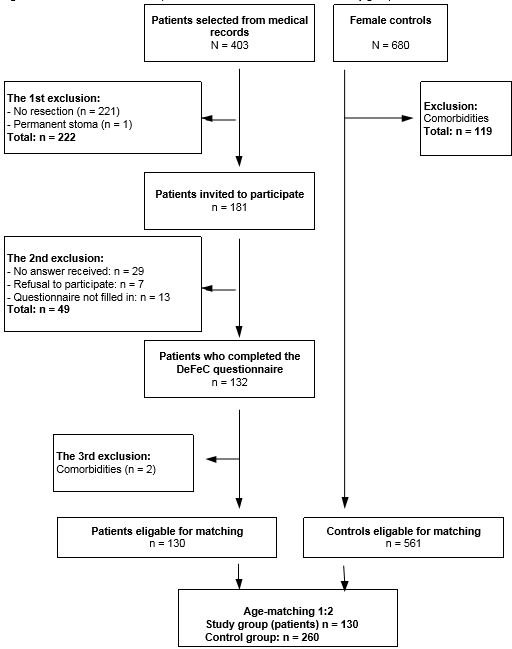
First, we screened the medical records of all patients diagnosed with endometriosis between January 2005 and December 2015 (Figure 1). The indications to operate women with DIE were unbearable abdominal and pelvic floor pain and problems with severe bleeding and/or fertility, and the fact that the patients could not have been helped with non-surgical treatment.
Stage IV endometriosis was defined according to the guideline of the American Society for Reproductive Medicine (ASRM), which is ‘’the presence of deeply invasive endometriosis with moderate to extensive adhesions between the uterus and bowels’’ [15]. All Patients (403) underwent either the pre-surgical Magnetic Resonance Imaging (MRI) at which (recto) sigmoid infiltration was evaluated by the radiologist or diagnostic laparoscopy during which endometriosis lesions in the (recto) sigmoid region were investigated, respectively. After multidisciplinary counseling, patients were subsequently seen in an outpatient appointment, at which point informed consent was taken, all the patients were explained the possible treatment options, their advantages and disadvantages. Optimal pre-surgical work-up was discussed at a multidisciplinary setting, including radiologist, colorectal surgeon and gynecologist. Furthermore, during surgical treatment, biopsies were taken from all patients and endometriosis was pathologically proven.
We initially excluded 221 women who had received endometriosis treatment other than (recto) sigmoid resection and one woman who had a permanent stoma. We invited 181 patients who had received laparoscopic (recto) sigmoid resection surgery at least a year before this study. Both segmental- and discoid (recto) sigmoid resections were included.
Out of the 181 patients, 145 agreed to participate. Of these, 132 patients filled out the DeFeC questionnaire. One woman suffering ulcerative colitis and one woman having Crohn’s disease were excluded. None of the patients reported other somatic diseases that could influence their bowels, such as Diabetes Mellitus, prolapse of the rectum, cerebral hemorrhage or infarction (stroke), neurological conditions such as paraplegia or slow transit constipation. None of the patients reported hereditary conditions such as anal atresia or congenital anorectal malformation, Hirschsprung’s disease, sacrococcygeal syndrome and spina bifida. Also patients who had previously undergone bowel surgery that may have affected their bowel function (e.g. perianal fistula, the anal sphincter or hemorrhoids), were excluded.
Finally, our patient group consisted of 130 women. We distinguished two subgroups: one consisted of the patients who had been treated less than 24 months ago (n=23) and the other of the patients who had been treated longer than 24 months ago (n=107).
Control Group
We used the database of the general Dutch population that had been compiled for our previous studies in 2015 [16]. We retrospectively used data on 680 women who had anonymously completed the digital DeFeC questionnaire. For this study, we chose to select a theoretically ‘’healthy’’ control group by excluding 119 respondents who reported the aforementioned diseases that may influence the bowel function. Subsequently, our control group consisted of 561 women.
For the analysis, we randomly age-matched the patients with women in the control group at a 1 to 2 ratio. The final control group consisted of 260 women. Women who underwent vaginal or any other type of child delivery were not excluded, which we corrected for by using multivariate analysis.
Data Analysis
Determination of constipation, fecal incontinence, Low-Anterior-Resection-Syndrome score and IBS
Constipation was determined according to the Rome IV criteria that consist of the following items: >25% defecation straining, lumpy, or hard stools, incomplete evacuation, anorectal blockage, manual maneuvers to support defecation, <3 spontaneous bowel movements per week, loose stools are rarely present without prior use of laxatives and insufficient criteria for IBS. To meet the criteria for constipation the respondents had to comply with at least two of these criteria for the last three months with symptom onset at least six months prior to diagnosis [17].
FI was also determined according to the Rome IV criteria, i.e. recurrent involuntary passage of fecal material (solid or liquid stool), including soiling, which occurs at least two to four times during four weeks for the last six months [17]. We also determined certain types of FI. Soiling was characterized by staining of underwear or the loss of small chunks of feces. Urge FI was defined as involuntarily losing of some, or substantial amounts of stool once urge sensation had been reached, but incapable of reaching the toilet on time. Liquid stool FI was defined as involuntary loss of watery stools or diarrhea and solid stool FI as involuntary loss of large amounts of solid feces, irrespective of urge sensation.
In addition, we determined the patients’ Low-Anterior-Resection-Syndrome (LARS) score [18]. Where 0-20 score indicated no LARS, 21-29 indicated minor LARS and 30-42 indicated Major LARS.
We also used the Rome IV criteria to determine IBS according to the following items: recurrent abdominal pain, on average, at least one day a week during the last three months and associated with two or more of the following: defecation, a change in stool frequency, and a change in appearance of stool. Respondents had to comply with at least two of the aforementioned criteria to meet the criteria for IBS [17].
IBM SPSS Statistics, Version 23.0 (Armonk, NY, USA: IBM Corp.) was used for statistical analysis. Descriptive statistics were used to characterize the respondents’ demographic characteristics and prevalences. We presented nominal variables as percentages and continuous variables as median and range. Comparisons were made using the chi-square test in case of categorical variables. Mann-Whitney U was used in case of continuous data. Univariate and multivariate regression analyses were used to determine the odds ratios (ORs) with the corresponding 95% CI. The level of statistical significance was set at a probability of <0.05. Microsoft Visio was used to create figures.
Ethical Approval
The study was approved by the Medical Ethical Committee of University Medical Center Groningen. All patients gave their written informed consent.
Characteristics of Patients and Control Group
The median age of the patients at the time of completing the questionnaire was 39 years (range 27-52 years) and 41 years (range 24-55 years) for the control group (P = 0.083). The median time between the (recto) sigmoid resection and completing the questionnaire was 52 months (range 14 - 139 months). The prevalence of vaginal deliveries among the patients was significantly lower compared to the control group (27.7% versus 46.5%, P = 0.001). Out of the 130 patients, 103 (79.2%) had segmental (recto) sigmoid resection and 27 (20.8%) had discoid (recto) sigmoid resection. We found that the prevalence of constipation and FI was not significantly different in patients who had undergone either resection procedure (P = 0.577 and P = 0.492). The median LARS score did not differ either between the patients treated with segmental (recto) sigmoid resections in comparison to those who had discoid (recto) sigmoid (21.0 versus 22.0, P = 0.542). As a consequence, we did not distinguish between the two resection procedures for the rest of the analyses.
Prevalence of Constipation and Its Symptoms
The prevalence of constipation in the patients who had undergone (recto) sigmoid resection for DIE was significantly higher than in the control group (50.8% versus 26.2%, P <0.001), Table 1.
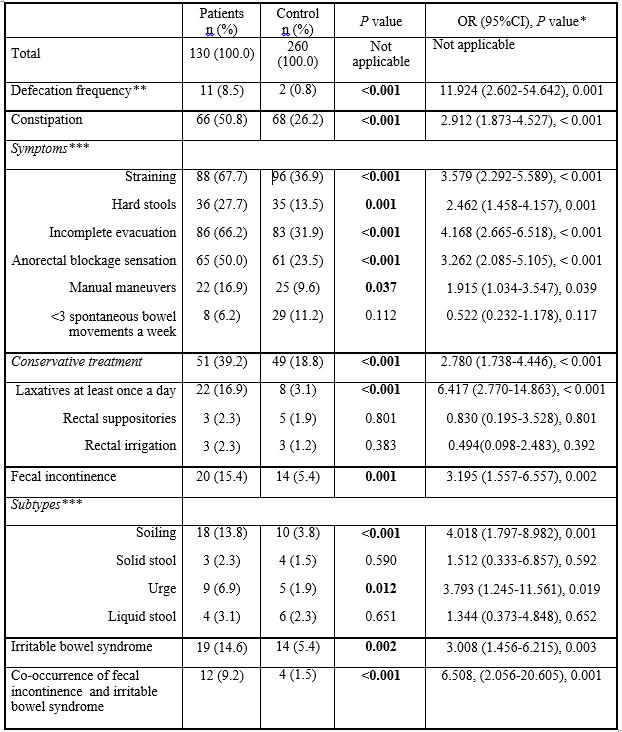
Abbreviation: OR - odds ratio; CI – confidence interval
*For the ORs the control group was used as reference; ** > Five times a day for the last six months; ***Some patients suffered from a combination of specific subtypes. Statistically significant differences are indicated in bold font.
Regression analysis confirmed that the patients were almost three times more likely to be constipated than the controls. The OR was 2.9 (95% CI, 1.873-4.527, P <0.001). The prevalence of constipation was also higher in the subgroup of patients treated less than 24 months ago in comparison to the subgroup treated longer than 24 months ago (69.9% versus 46.7%, P = 0.065). The OR was 2.606 (95% CI, 0.992-6.846, P = 0.052). Nevertheless, the prevalence of constipation of both the subgroups remained significantly higher than in the control group (69.9% versus 26.2%, P <0.001 and 46.7% versus 26.2%, P <0.001), as was the likelihood of constipation (OR=6.085, 95% CI=2.403-15.408, P<0.001 versus OR=2.335, 95%, CI=1.463-3.727, P <0.001).
The prevalence of the symptoms that are usually associated with constipation, analyzed as an independent symptom, was also significantly higher in the patient group: straining (P <0.001), hard stools (P = 0.001), incomplete evacuation (P <0.001), anorectal blockage sensation (P <0.001), and manual maneuvers (P = 0.037), Table 1. Additionally, the patients were almost three times more likely to use laxatives and other forms of conservative treatment than the control group. The OR was 2.8 (95% CI, 1.738-4.446, P <0.001).
Prevalence of Fecal Incontinence and Its Symptoms
We also found that the prevalence of FI after (recto) sigmoid resection for DIE was significantly higher than in the control group (15.4% versus 5.4%, P = 0.001), Table 1. Regression analysis confirmed that the women with DIE were three times more likely to have FI than the controls. The OR was 3.2 (95% CI, 1.557-6.557, P = 0.002). The prevalence of FI between the subgroup of patients treated less than 24 months ago and the subgroup treated longer than 24 months ago was comparable (17.4% versus 15.0%, P = 0.769). The OR was 1.197 (95% CI, 0.360-3.983, P = 0.769). The prevalence of FI in both subgroups remained significantly higher than in the control group (17.4% versus 5.4%, P <0.001 and 15.0% versus 5.4%, P <0.001 ) as was the likelihood of FI (OR = 4.000, 95% CI=1.188-13.467, P = 0.025 versus OR=3.341, 95% CI=1.546-7.217, P = 0.002). When looking at two forms of FI, we found that soiling FI and urge FI were significantly more frequent in the patient group than in the control group (P <0.001 and P = 0.012), Table 1.
The Co-Occurrence of Constipation and Fecal Incontinence
The prevalence of FI in constipated patients was significantly higher in comparison to the constipated control group (9.2% versus 1.5%, P <0.001), Table 1. Regression analysis confirmed this observation. The OR was 6.5, (95% CI, 2.056–20.605, P = 0.001).
Prevalence of Irritable Bowel Syndrome
The prevalence of IBS among patients after (recto) sigmoid resection for DIE was significantly higher than in the control group (14.6% versus 5.4%, P = 0.002), Table 1. Univariate regression analysis confirmed that the patients were at higher risk of having IBS than the control group. The OR was 3.0 (95% CI, 1.456-6.215, P = 0.003).
Low Anterior Resection Syndrome Score
The median LARS score was also significantly higher in the patients than in the healthy controls (21.5 versus 16, P <0.001, Table 2).
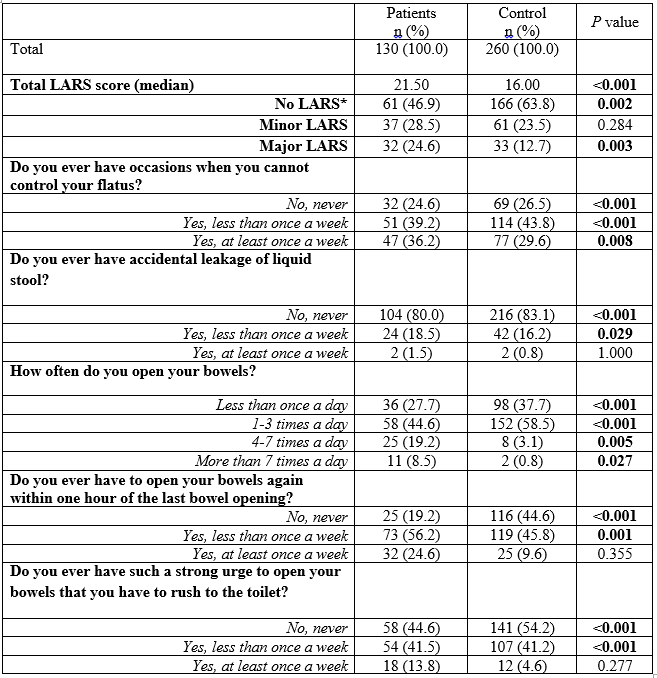
Abbreviations: LARS – Low Anterior Resection Syndrome.
* 0-20 no LARS; 21-29 minor LARS; 30-42 major LARS
The controls had a LARS score between 0–20, indicating no LARS, significantly more often than the patients (63.8% versus 46.9%, P = 0.002). More importantly, the prevalence of major LARS was significantly higher in the patient group (24.6% versus 12.7%, P =0.003). In addition, most of the symptoms characteristic of LARS were significantly more frequent in the patients than in the controls. The median LARS score was higher in the subgroup of patients treated less than 24 months ago in comparison with the subgroup treated longer than 24 months ago (24.0 versus 20.0, P = 0.245). There was no difference
between major LARS in either subgroup (21.7% versus 25.2%, P = 0.203), however, absence of LARS was significantly more prevalent in the subgroup treated longer than 24 months ago (50.5% versus 30.4%, P = 0.041).
Risk Factors Associated With Constipation and Fecal Incontinence
Being a patient was the only significant factor associated with constipation, Table 3.

Abbreviations: DIE – deep infiltrating endometriosis; FI - fecal incontinence; IBS – irritable bowel syndrome;
OR - odds ratio, CI – confidence interval
Statistically significant findings are indicated in bold font.
1 Patients with DIE versus controls
2 Patients with IBS versus controls with IBS
3 for this analysis patients with IBS were excluded
4 Patients and controls with at least one vaginal delivery
For FI, both univariate and multivariate analysis revealed that being a patient and having IBS significantly increased the risk of FI. Because IBS increased the risk of FI by six times, we additionally performed an analysis whereby we excluded patients and controls with IBS. Still, being a patient, surgery for DIE significantly increased the risk of FI by more than two (P = 0.043). Interestingly, patients and controls who had given birth vaginally were less likely to develop FI (OR = 0.26, P = 0.011). Multivariate analysis with vaginal delivery and IBS as covariates, showed that being a patient significantly increased the risk of developing FI.
In this study, we show that the postoperative outcomes regarding defecatory disorders, including constipation, FI, their co-occurrence, IBS, and associated symptoms are still far from optimal in patients who underwent (recto) sigmoid resection for DIE, as confirmed by comparison with a control group.
The clinical improvement of patients having surgery for DIE has already been reported before [10, 11]. We show however, that these patients, despite the treatment, still have significantly higher risks of suffering from constipation than women who had never experienced DIE. Consequently, also a broad spectrum of constipation-associated symptoms have been reported by at least half the patients. These include incomplete defecation, anal blockage, hard stools, and straining. Finally, relatively frequent manually supported defecation, or laxative use, also indicate suboptimal outcomes in the patients. Additionally, constipation is known to be a risk factor for FI [19], and indeed, the patients in the current study experienced FI approximately six times more often than non-patients. The high prevalence of different forms of FI, including soiling and urge FI in patients, is also notable, especially when we realize that it is approximately three times higher than in the control group.
Furthermore, it is known that the time of regeneration can contribute to improved postoperative outcomes [10, 11]. Indeed, patients who had undergone surgery more than 24 months before the survey have better outcomes in terms of constipation than patients treated less than 24 months before, albeit not in the case of FI. It seems thus that the period of postoperative regeneration of the pelvic floor may only contribute partially to the improvement of bowel functions.
IBS is also a known risk factor for FI [20-22], and our patients experience IBS more often than the non-patients. We did, however, find that patients who do not experience IBS, still have a more than two times higher risk of having FI than controls. This indicates that IBS is not the only factor that has contributed to the increased prevalence of FI in our patients.
It is known that after low anterior resection patients can develop LARS, and constipation or FI belong to the most typical symptoms of LARS [23-25]. As shown recently, LARS can also be present in the general population [26]. Nevertheless, patients from our study experience Major LARS significantly more often than controls. Vaginal delivery too is often considered a risk factor for developing FI [27-30]. Although we corrected for this cofactor in our analysis the outcomes regarding FI have not changed.
The findings we describe illustrate that although the postoperative outcomes of patients suffering from DIE are known to improve, the patients’ condition remains far from optimal compared to healthy controls.
With this study, researchers were unable to establish the direct causes of the suboptimal postoperative outcomes regarding patients’ bowel functions. The defecatory disorders could already have existed before the patients developed DIE, because such disorders also occur in the ‘healthy’ population [26]. The causes could have developed or could have become progressively worse along with the growth of endometriosis. One might also imagine that the surgical intervention caused damage to the pelvic floor and that it influenced bowel functions negatively. Studies reporting on improved postoperative outcomes compared to the preoperative situations, allowed us to reject this possibility [10, 11].
That we did not use a preoperative baseline for our patients might also be seen as a limitation. Such studies, however, have already been performed. Moreover, the preoperative baseline would not have enabled us to answer our question about how far removed patients treated for DIE were from ‘normal women’, that is women who never suffered endometrioses. The ideal baseline would consist of patients before they had DIE, but this is rather difficult to determine. Different diagnostic tests should be performed to diagnose the possible functional causes of postoperative constipation, FI, or IBS. We think that symptoms related to defecatory disorders, including chronic abdominal pain [4], abdominal bloating, painful bowel movements, and painful defecation experienced before treatment for DIE, might in some patients have contributed to inadequate use of their pelvic floor muscles, resulting in dyssynergic defecation [31]. Surgery for DIE removed endometriosis, reduced pain, but it did not remove prior symptoms that, as we demonstrated, still occurred frequently in the patients after surgery. Thus, poor preoperative conditions could have contributed to suboptimal postoperative outcomes.
Patients who underwent (recto) sigmoid resection for DIE are at a significantly higher risk of suffering constipation, FI, and IBS than women who have never experienced DIE. Despite postoperative outcomes of patients treated for DIE improving after 24 months, patients are still far from optimal in comparison to controls. This finding should encourage medical specialists to postoperatively screen their patients for the possible bowel problems, offer adequate treatment when necessary, and in this way, offer a complete care. Moreover, although indirectly, this data adds to the knowledge regarding the cause of the abdominal pain, which belongs to the most frequent criteria to operate patients with DIE; Since constipation can present with a severe abdominal pain, it is possible that a certain cohort of patients diagnosed with DIE and operated due to the abdominal pain, had suffered from constipation already before the (recto) sigmoid resection. Consequently, it is possible that some of the patients might have been helped with non-surgical, conservative treatment for constipation. Following this rationale, we conclude that patients suffering from DIE and suffering severe abdominal pain, should be screened for bowel disease before the decision about surgery is taken.
Patients should be advised by an experienced medical specialist to undergo diagnostic tests before making decision about surgery to exclude that certain symptoms, for instance abdominal pain, result from a pre-existing bowel dysfunction. Furthermore, medical specialist should take care of postoperative screening of bowel function of their patients, and when necessary, establish the cause of their suboptimal bowel functions and provide with suitable treatment.
Acknowledgements
The authors would like to thank RoQua, University Medical Center Groningen, Groningen, the Netherlands, and particularly Ellen Visser, PhD, for invaluable assistance during the completion of this survey. We also extend our gratitude to Froukje Hoogenboom, MD, for constructive advice while drafting the manuscript.
The content of this manuscript was presented at the following meetings:
Poster presentation at the meeting of the European Society of Human Reproduction and Embryology, 1-4 July 2018, Barcelona, Spain.
Poster presentation at the meeting of the The Society of Endometriosis and Uterine Disorders, 26-28 June 2018, Florence, Italy.
Oral presentation at the meeting of the European Society for Gynaecological Endoscopy, 7-10 October 2018, Vienna, Austria.
Declarations
Funding: none
Conflicts of interest: none
Author Contributions:
Study concept and design: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens
Acquisition of data: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens
Analysis and interpretation of data: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens
Drafting the manuscript: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens
Critical revision of the manuscript for important intellectual content: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens
Statistical analysis: Al-Saidi and Trzpis
Final approval of the version to be published: Al-Saidi, Klinkert, Hofker, Trzpis, and Broens.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
